Abstract
Background: Hirsutism is a common problem for
which laser is being the treatment of choice. Several lasers
with varying wavelengths, pulse durations, energy fluences
and skin cooling systems, are currently used for hair
removal. However, the ideal laser parameters and group of
patients who respond better after treatment remain largely
unknown. Objectives: A prospective study to evaluate the
long term efficiency and safety of three different (Ruby,
Alexandrite, Diode) laser hair reduction systems and to
determine which candidates respond better for hair
reduction.
Methods: 171 female patients with Fitzpatrick skin
types II- IV with the problem of hirsutism, in the beard area
were divided into three groups. Group one included 60
patients, who were treated by ruby laser; group two included
51 patients who were treated by Alexandrite laser whereas
the third group included 60 patients who were treated by
diode laser. Detailed history, Hormonal assay and abdomino-pelvic
ultrasonography were performed to differentiate between
idiopathic and pathological hirsutism. Treatment was
performed in multiple sessions with an interval of 4 weeks
using either: ruby laser, long pulsed Alexandrite laser or
diode laser. Hair thickness and rate of hair reduction and
re-growth were recorded by using Hair counts and photographs
before treatment and after 1,3,6,9 &12 months from the
initial treatment.
Results: All patients had reduction in hair count and
delayed hair re-growth. Patients less than 30 years of age
responded better than those more than 30 years regardless of
the other clinical factors or the type of laser used. There
was a significant statistical difference between them at 6
and 12 months follow up (P< 0.05).Patients with hirsutism
due to any underlying cause responded as the idiopathic
ones. Medical treatment (antiandrogen drugs) during the
course of laser sessions had no role in improving the
results. Concerning laser parameters, the three lasers used
were found to have positive results in hair reduction.
Conclusion: The three types of lasers showed variable
degrees of improvement concerning the percentage of hair
reduction and the rate of hair re-growth. The best results were
obtained with diode followed by the Alexandrite. Ruby laser
produced the poorest results. The least complications were
observed with the diode laser, followed by the Alexandrite.
Age plays an important role in the efficacy of laser hair
removal diode laser proved to be the most effective and
safest laser in this study.
Introduction
Hirsutism is defined as the growth of terminal
hair in a woman in sites at which it is usually considered a
male secondary characteristic e.g. chin and beard area. The
severity of hirsutism depends on the underlying disorder
resulting in excess production or increased availability of
the potent or weak androgens (testosterone,
dehydroepiandrosterone (DHEA) and androstenedione).
Hirsutism may result from ovarian and/or
adrenal overproduction of androgens or some exogenous
medications. Polycystic ovarian syndrome is the underlying
disorder in the majority of women who present with hirsute.
It is characterized by a typical ultrasound appearance of
the ovaries and a variable endocrine and clinical picture [1].
Hirsutism may be idiopathic, due to androgen
receptors hypersensitivity, or hereditary. It may result
from an increased end organ ability to produce
dihydrotestosterone (DHT) from weaker androgens.
Many temporary hair removal methods exist, including
shaving, tweezing, wax epilation and chemical depilatories.
Most of these methods are tedious, others are invasive or
time consuming such as Electrolysis and thermolysis or take
a long time to produce an effect. Other methods may
interfere with hormonal profile or desire for pregnancy such
as antiandrogens. The need for a rapid, permanent reduction
and noninvasive method for hair removal has led to the
development of various lasers. Hair removal lasers generally
work on the principle of selective photothermolysis, based
on selective absorption of laser energy by the components of
the hair follicle. The target chromophore is melanin
contained by the follicle, which has a broad absorption
spectrum. Several lasers with different wavelengths have
been able to take advantages of this approach. These lasers
range from the short end of the spectrum with 694 nm ruby
laser[2],
to the middle, with the 755 nm Alexandrite[3] and 810 nm
diode[4], to the long end with the 1064 nm Nd;YAG laser[5].
The laser Wavelength determines both the amount of energy
absorbed by the target and the surrounding tissue in
function of their color/pigment and the depth of
penetration. In addition to wavelength, effective fluence
(the fluence delivered at the target depth) is also
influenced by the spot size and pulse width. Larger spot
sizes and longer wavelengths are more efficient at
delivering a greater proportion of their energy to target
tissues as the depth of the target increases [6]. Pulse width
is the amount of time (in milliseconds) over which the total
energy (in joules) contained in one pulse is delivered to
the surface of the skin. For hair removal, the optimum pulse
duration is approximately equal to the thermal relaxation
time (TRT) of the hair follicle. The TRT is defined as the
time required for an object to cool to half the temperature
achieved immediately following laser exposure. For human
terminal hair, TRT varies from about 10 to 100 milliseconds
[7].
Even laser light with selective photothermolysis and perfect
specificity for melanin can cause damage to the skin
surrounding the hair follicles, as the epidermis also
contain melanin. The use of an epidermal cooling strategy,
allows the delivery of sufficient laser energy to damage the
hair follicle while avoiding and minimizing damage to the
surrounding skin.
Patients and methods
171 hirsute female patients with Fitzpatrick
skin types II-IV were included in this study. Their ages
ranged from 17-50 years (mean 32 years). Informed consent
had been obtained from each patient prior to treatment. The
area studied was the beard, even if there were other areas
affected and treated.
Comprehensive history and examination were
performed in order to detect any hormonal disturbance or
underlying disorder, if any leading to growth of excess
hair.
Abdomino-pelvic sonography and Hormonal assay were done as a
routine investigation. These included level of Testosterone,
Dehydroepiandrosterone sulphate (DHEA-S), plasma Cortisol
and Prolactin.
Treatment was performed using either one of 3
types of lasers. The first group were exposed to ruby laser
(EpiTouch Silk, Sharplan) at 694 nm and 1.2 ms pulse
duration, at fluences of 25-40 J/cm2 through different spot
size (3,5,6mm). The second group were exposed to Long pulsed
Alexandrite laser (LPIR, Cynosure) at 755 nm and 20 ms pulse
duration, at fluences of 10-25 J/cm2 (average 20 J/cm2)
through 7-10 mm spot size at 1 Hz. The third group was
exposed to diode laser (Light Sheer, Star Med / Coherent) at
800 nm and 5-30 ms pulse duration, at fluences of 10-40
J/cm2 through a 9 mm spot size at a repetition rate 1-2
pulses/ sec. Fluence was determined, prior to the initial
treatment session, by the maximum fluence tolerated
according to the patient pain threshold and by the minimal
resulting erythematous reaction, without any evidence of
burn.
Treatment was done in multiple sessions with an
interval of 4 weeks and continued till a patient
satisfactory hair count was reached or hair reduction ceased
in two consecutive sessions.
In case of ruby and Alexandrite lasers, a
cooling gel or ice packs were applied to the skin surface
few seconds before and after treatment. In case of diode
laser, the integrated sapphire contact cooling hand piece
was used.
Post operative care for all patients included
applying ice directly following laser sessions for a few
minutes, sun avoidance, prophylactic topical antibiotics and
sun screen cream with SPF 30 or more.
All patients were instructed to leave the hair
unshaved ten days prior to treatment and to stop hair
removal methods apart from shaving or using depilatory cream
between sessions. Areas of unwanted hair growth were
identified and marked. It was measured using a transparency
grid divided into equal squares; the area of each is 1 cm2.
The terminal hairs in 10 squares were counted and the mean
was calculated every time.
The differences between the mean before
treatment and at 1, 6, and 12 months periods were
determined. The primary outcome measure was the percentage
of hair reduction, defined as the percentage of each
difference with respect to the initial hair count before
treatment. Other secondary outcome measures were the rate of
hair regrowth, complications including hyperpigmentation,
white hair and recurrence.
Results
The clinical characteristics for the three
groups were comparable (table 1).
The mean number (mean +/- SD) of treatment sessions in the
idiopathic hirsutism group were 6.33 +/- 1.2, 4.03 +/- 2.08
and 3.56 +/- 1.21 for the ruby, Alexandrite and diode groups
respectively. In the pathologic hirsutism group, they were
6.10 +/- 1.29, 4.60 +/- 2.32 and 3.58 +/- 1.32 respectively.
An immediate erythematous skin response was observed in all
laser treated beard areas. All laser treated areas displayed
a delay in hair regrowth. The results recorded for patients
treated and followed up for 6 and 12 months revealed
generally that patients whose ages were less than 30 years
gave better response for laser treatment than those whose
ages were more than 30 years regardless the other clinical
factors and the type of laser used (Table
1). There was a significant statistical difference
between them at 6 and 12 months follow up (P < 0.05). The
best results were obtained when diode laser was used. In this case there was also a significant
statistical difference between those of age less than 30
years and those above 30 years at 6 months follow up (P <
0.05). Poor response was observed when ruby laser was used.
Polycystic ovarian syndrome accounted in 20% of the causes
of hirsutism (35 out 171). There were no significant
statistical differences between patients either with or
without hormonal disturbance, polycystic ovary, family
history and taking medical treatment in the form of
antiandrogens during laser sessions on percentage of hair
reduction. The results shown in table 2 indicate that there was no significant
difference in the response between idiopathic patients and
pathological groups. However, better results were obtained
when diode laser was used for treatment.
 |
 |
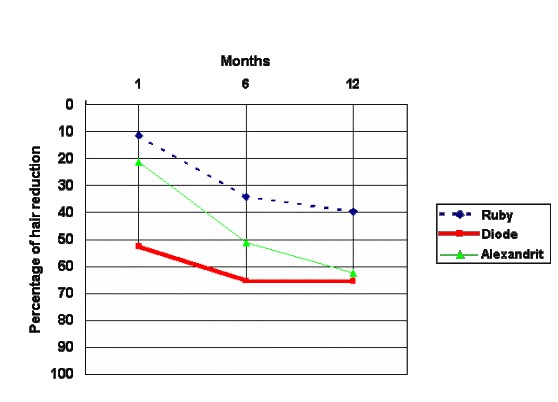
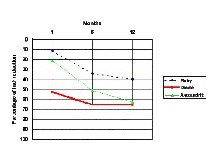
| Fig. 1:
Percentage of
Hair Reduction at 1, 6 and 12 months follow up |
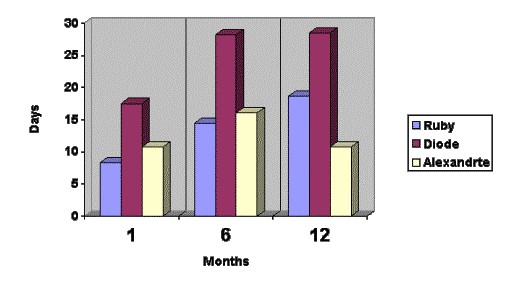
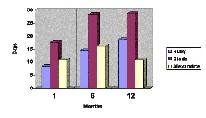
Fig. 2:
Percentage of Hair Regrowth at 1 , 6 and 12 months follow up. |
 |
 |
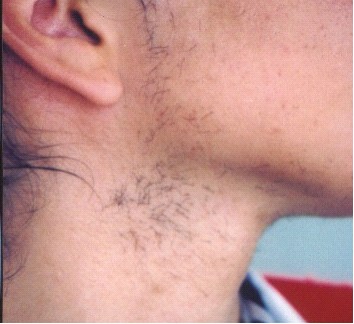
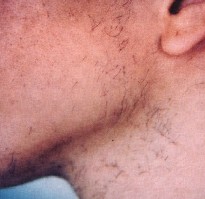
| Fig 3a:Left side before treatment. |
Fig 3b: Same side after ruby laser treatment . |
 |
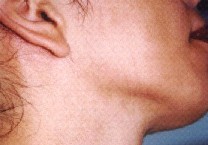 |
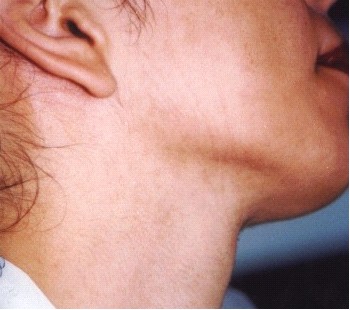
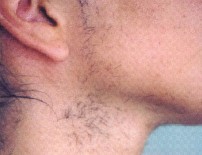
| Fig. 4a: Right side of the patient before treatment. |
Fig. 4b: Same side after diode laser treatment. |
 |
 |
| Fig. 5a: Before treatment. |
Fig. 5b: After Alexandrite laser treatment |
Discussion
In this study the diode laser induced a
significant rapid reduction of hair growth that increased on
long term follow up. The percent of hair reduction was
significantly the least in the ruby group, 11.25, 20.17 and
39.67 percent at one, six and 12 months respectively.
Alexandrite laser gave results (21.08, 51.08 and 62.35
respectively) intermediate between those obtained with diode
and ruby laser. In addition, the duration of hair re-growth
was shortest in the ruby group and longest in the diode
group.
The results of our study showed marked
correlation between the percentage of hair reduction due to
laser treatment and patient's age irrespective of the
underlying pathology. Patients below 30 years of age
responded better than older patients. This does not agree
with the findings of Liew et al, where they reported no
correlation between the efficacy of ruby laser treatment and
age [2].
The age related improvement may be explained by the
increased tyrosinase activity in middle age, which is
responsible for formation of the end product melanin
chromophore, through the production of an intermediate
compound, dopaquinone, from the precursor tyrosine [8]
The lack of any significant statistical
difference between the response of pathological groups and
idiopathic groups suggests that the inherent susceptibility
of hair to laser irradiation is more important in hair
destruction than the physiology of hair growth [9].
It is interesting to note that medical treatment in the form
of anti-androgens did not improve nor accelerate laser
treatment response. This finding conform to Lumachi ,
Rondinone, report [10]
as anti-androgen drugs have only a suppressive and not
curative effect that wears off a few months after cessation
of therapy.
This study included the largest number of
treated subjects who were followed for long duration. Other
studies showed a reduction in hair growth after 2 years,
however the patients number was too small [11].
Other prospective controlled studies had either a smaller
number of subjects or shorter follow up duration [12].
In the current study, the evaluation was done
objectively by measuring the percentage of hair reduction
and rate of hair re-growth, by counting the hairs through a
transparency grid. Other studies based their evaluation on
either subjective assessment or histo-pathological
evaluation). The invasive histological evaluation, used by
others [9]
would have been unacceptable in our study, in the beard
area, for cosmetic reasons.
Other studies measured the change in hair
diameter using very sophisticated computerized image
analysis systems [13].
The evaluation in our study was simple, objective and can be
repeated.
However, in our study the sessions were
continued till a patient satisfactory hair count was reached
or hair reduction ceased in two consecutive sessions. This
is different from Most published studies were the response
was studied after a pre set number of treatment sessions.
The results obtained in our study represent the
maximum benefit that can be gained from the treatment.
Despite that the rate of hair reduction in Alexandrite and
diode groups was nearly equal at 12 months, the diode laser
proved be more effective, as the number of sessions were
fewer.
Other studies reported improvement in the
treatment of aesthetic hair or looked at many sites [9].
Our study assessed the pathological and looked at one site.
It is the largest study assessing the hirsutism in the beard
area, the most distressing site in women, where it is thick,
coarse with short anagen duration. These are expected to
have a different response to laser treatment.
A variety of factors had influenced the results
of hair reduction between the three laser systems. Ruby
laser (694nm) produced the poorest result in this study
despite it is the most absorbed by the chromophore melanin.
This can be explained by fact that the longer the
wavelength, the greater depth of penetration.
The Alexandrite and diode lasers (at
Wavelengths of 755 nm and 800 nm respectively) have 1-1.5 mm
greater depth of penetration than the ruby laser and exert
their effect on the hair follicle by applying the principles
of selective photothermolysis. These Wavelengths are able to
penetrate deep into the dermis and selectively target
follicular melanin [14]. In addition, the used 20 msec pulse
duration of Alexandrite and 30 msec pulse duration of diode
laser in this study lie above the thermal relaxation for the
epidermis, which is estimated to be 3-10 msec and below the
thermal relaxation time of the hair follicles, which is
estimated to be 40-100 msec, thereby optimizing selective
destruction of hair follicle.
In this study the shortest ruby laser pulse
duration (1.2 msec) was used. Changing pulse duration may
affect the response to the ruby laser. Long duration pulsed
ruby lasers were recently developed.
The better results obtained with the diode
laser may had been enhanced partly by the cooling effect of
the integrated sapphire and the pressure exerted by it on
the skin. Sapphire is ideal, as it has excellent thermal
characteristics and operates as a heat sink removing heat
from the epidermis[15]
This enables the target structures to be heated more
efficiently, so that less fluences are required, resulting
in less thermal load on the epidermis[16].
The latter effect is not present in the other two lasers
where only cooling without pressure effect was exerted.
The possibility of using a larger spot diameter
in the diode and Alexandrite lasers adds the advantage of
covering a larger area over a short time, and also increases
the depth of penetration.
Our findings confirm the value of laser in hair
reduction in the beard area of patients with Fitzpatrick
skin types II - IV. In our study series of 171 patients that
extended over 12 months, there were very few complications
in the form of hyperpigmentation, white hair and recurrence.
The best results were obtained with diode followed by the
Alexandrite. Ruby laser produced the poorest results. The
least complications were observed using the diode laser,
followed by the Alexandrite. The highest rates of
complications occurred in the ruby group (6.7 to 8.3).
Accordingly ruby laser is no longer used in the management
of hirsutism in our center and diode laser has become the
laser of choice. Although we are much encouraged by the hair
reduction in hirsutism by the diode and the Alexandrite
laser, this work only studied the beard area. Further study
on other body sites in hirsutism is needed.
References
1. Falsetti L, Gambera A, Andrico S, Sartori E. Acne and hirsutism in polycystic ovary syndrome: clinical, endocrine-metabolic and ultrasonographic differences. Gynecol Endocrinol. 2002 Aug;16(4):275-84.
2. Liew SH, Ladhani K, Grobbelaar AO, Gault DT, Sanders R, Green CJ, Linge C. Ruby laser-assisted hair removal success in relation to anatomic factors and melanin content of hair follicles. Plast Reconstr Surg. 1999 May;103(6):1736-43.
3. Garcia C, Alamoudi H, Nakib M, Zimmo S. Alexandrite laser hair removal is safe for Fitzpatrick skin types IV-VI. Dermatol Surg. 2000 Feb;26(2):130-4.
4. Sadick NS, Prieto VG. The use of a new diode laser for hair removal. Dermatol Surg. 2003 Jan;29(1):30-3; discussion 33-4.
5. Weaver SM 3rd, Sagaral EC. Treatment of pseudofolliculitis barbae using the long-pulse Nd:YAG laser on skin types V and VI. Dermatol Surg. 2003 Dec;29(12):1187-91.
6. Ross EV, Ladin Z, Kreindel M, Dierickx C. Theoretical considerations in laser hair removal. Dermatol Clin. 1999 Apr;17(2):333-55, viii. Review.
7. Anderson RR, Parrish JA. photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983 Apr 29; 220 (4596).
8. Grossman M.C. Hair removal, From: Cutaneous laser Surgery. Second edition, Edited by: Goldman MP and Fitzpatric R.E, chapter 5, P. 259-278. Mosby Inc., Boston, New York, London and Toronto, 1999.
9. Liew SH, Ladhani K, Grobbelaar AO, Gault DT, Sanders R, Green CJ, Linge C. Ruby laser-assisted hair removal reduces the coarseness of regrowing hairs: fallacy or fact? Br J Plast Surg. 1999 Jul;52(5):380-4.
10. Lumachi F, Rondinone R. Use of cyproterone acetate, finasteride, and spironolactone to treat idiopathic hirsutism. Fertil Steril. 2003 Apr;79(4):942-6.
11. Dierickx CC, Grossman MC, Farinelli WA, Anderson RR. Permanent hair removal by normal-mode ruby laser. Arch Dermatol. 1998 Jul;134(7):837-42.
12. Grossman MC, Dierickx C, Farinelli W, Flotte T, Anderson RR. Damage to hair follicles by normal-mode ruby laser pulses. J Am Acad Dermatol. 1996 Dec;35(6):889-94.
13. Fournier N, Aghajan-Nouri N, Barneon G, Mordon S. Hair removal with an Athos Nd:YAG 3.5 ms pulse laser: a 3-month clinical study. J Cutan Laser Ther. 2000 Sep;2(3):125-30.
14. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983 Apr 29;220(4596):524-7.
15. Eremia S, Li C, Newman N. Laser hair removal with alexandrite versus diode laser using four treatment sessions: 1-year results. Dermatol Surg. 2001 Nov;27(11):925-9.
16. Klavuhn KG, Green D. Importance of cutaneous cooling during photothermal epilation: theoretical and practical considerations. Lasers Surg Med. 2002;31(2):97-105.
© 2004 Egyptian Dermatology Online Journal